Anti-A1 and Anti-A2 IgM Antibodies in ABO Subgroup Testing
Comprehensive technical guide to Anti-A1 and Anti-A2 IgM antibodies in human blood typing. Covers A1 vs A2 subgroups, antibody detection methods, clinical significance, transfusion reactions, and genetic background.
How to detect Anti-A1 antibodies in transfusion medicine ?
Difference between A1 and A2 blood group antigens !
Clinical impact of Anti-A1 IgM in transfusion safety.
Gentaur
Scientific Publications
Anti-A1 and Anti-A2 IgM Antibodies in ABO Subgroup Testing
Anti-A1 / Anti-A2 IgM Blood Group Antibodies
The ABO blood group system is one of the most clinically important human blood typing systems. Within group A (and AB), the A antigen has subgroups: A1 and A2 are the most common. The existence of these subgroups gives rise to specific antibodies such as Anti-A1 and Anti-A2, typically of the IgM isotype. Understanding their properties, detection, clinical significance, and laboratory handling is essential for transfusion medicine, immunohematology research, and organ transplantation.
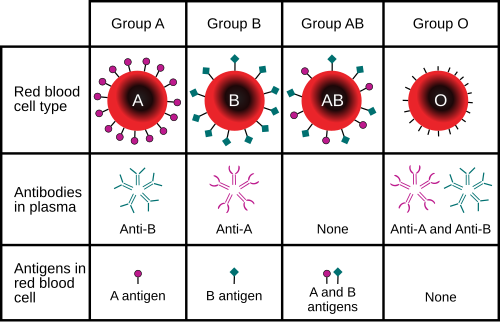
Basic Concepts : A1 vs A2 Subgroups
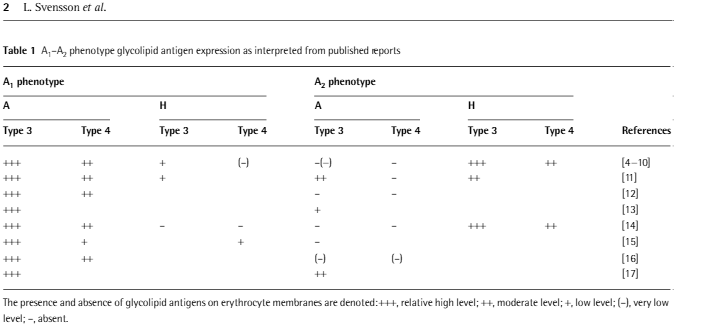
- Definition : The A antigen subgroups differ in the density and structure of A-antigen sites on red blood cells (RBCs). A1 has a higher number of antigen sites and “finer” structural variation; A2 has fewer sites.
- Frequency : In many populations, approximately 80 % of those with blood group A (or AB) are A1, while about 20 % are A2. For AB individuals, similar proportions (majority A1B, smaller portion A2B) are seen.
- Serologic identification : A1 cells react strongly with Anti-A1 lectin (often from Dolichos biflorus), whereas A2 cells do not react or react weakly. RBC panels including A1, A2 reagent cells are used in the lab to distinguish.
Anti-A1 / Anti-A2 Antibodies : Properties
Mechanism of Action
- Antibody binding : IgM anti-A1 attaches to A1 antigenic epitopes on RBC membranes. Because A2 cells express the A antigen at lower density and somewhat different structure, binding of anti-A1 to A2 is weak or absent except in rare broadened specificities.
- Complement activation : IgM is efficient in initiating the classical complement pathway, which can lead to hemolysis if antibody binding occurs at body temperature (37 °C) and the complement system is activated.
- Natural vs induced : Most anti-A1 antibodies are naturally occurring (i.e., appear without known immunization). Induced forms (after transfusion, pregnancy, transplantation) may have greater thermal amplitude / titer.
Detection & Laboratory Methods
Serologic testing :
- Reverse grouping / serum grouping : Testing patient plasma/serum against reagent RBCs of A1, A2, and O to see agglutination. If serum agglutinates A1 cells but not A2, anti-A1 may be present.
- Lectin tests : Use of Dolichos biflorus lectin which selectively agglutinates A1 cells. Helps distinguish A1 vs A2.
- Temperature and phases : Immediate spin at room temp, incubation at 37 °C, then anti-human globulin (AHG) phase to detect weaker or warm antibodies.
- Titration : Serial dilutions to establish highest dilution causing agglutination. Important to quantify strength.
Molecular genotyping :
- Genotyping of ABO alleles and subgroups can reveal A1 vs A2 at the genetic level, which may help in transplantation or in settings where serology is ambiguous.
Clinical Implications
Transfusion medicine :
*For A2 or A2B individuals with anti-A1, transfusing A1 blood may lead to minor hemolytic reactions if antibody is reactive at body temperature. Most labs avoid unnecessary risk.
*Compatibility testing should include A1, A2 reagents when discrepancy suspected.
Transplantation :
*In kidney / organ transplant, subgrouping (A2 vs A1) may allow more donor options (for example, A2 to B transplantation) because A2 antigens are less immunogenic. Genotyping helps.
ABO discrepancy resolution :
*Reverse grouping showing unexpected agglutination with A1 cells but not A or weak reaction may suggest anti-A1. Must rule out cold autoantibodies or irregular antibodies.
Risk assessment :
*Significance increases with high titer, reactivity at 37 °C, evidence of complement activation, or clinical signs of hemolysis.
Laboratory Guidelines & Best Practices
-Always include A1 and A2 reagent cells (or equivalent) in reverse typing panels when patient or donor is A or AB, to detect subgroup effects.
-Use Dolichos biflorus lectin for confirmatory subgrouping.
-When anti-A1 is detected :
- Determine titer of the antibody.
- Test thermal amplitude : does it react at 37 °C / in AHG?
- Assess for complement binding (e.g. via antiglobulin test, complement reagent).
-Transfusion decisions :
*If anti-A1 is cold reactive only, low titer, limited risk, A1 blood may be used cautiously.
*If warm reactive / high titer / complement activating, better to transfuse with A2 or O blood, or matched subgroup if possible.
-Documentation: Clearly record subgroup (A1 / A2), presence of anti-A1 or anti-A2, titer, thermal amplitude. This is critical for future transfusions / donor selection.
Summary & Conclusion
- Anti-A1 and Anti-A2 IgM antibodies are naturally occurring in many individuals, especially those with subgroup A2 or A2B.
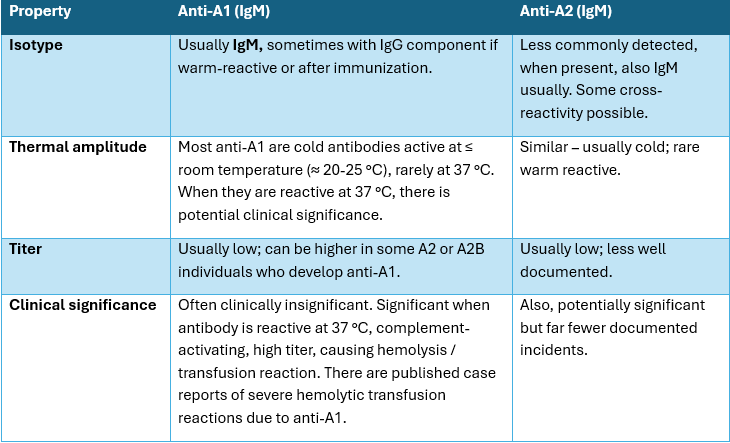
- Most anti-A1 are cold-reactive and clinically insignificant; rarer warm-reactive or high-titer forms can cause transfusion reactions.
- Accurate detection with proper reagent cells, lectins, titration, and thermal phase testing is crucial.
- Genetic subgrouping (A1 vs A2) adds precision, especially in transplantation or difficult serology.
- For patient safety : documenting subgroup, antibody presence, and characteristics is essential so that blood matching is appropriate.